In the picture: Rheoencephalogram of a young and healthy 34-year-old man
The explanation is only for those who are strictly interested!
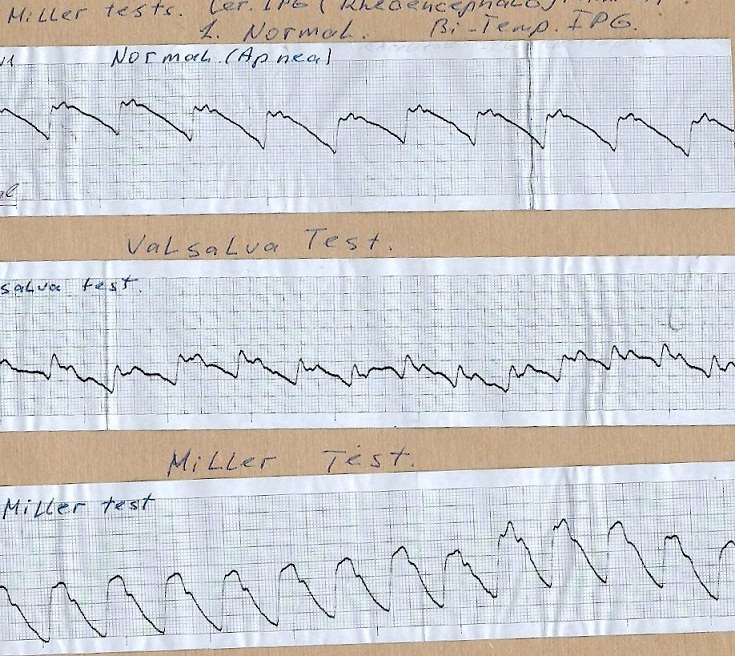
It is interesting to analyze these curves (Rheoencephalogram – REG). The subject was a young healthy man of 34 years old.
The upper recording is a normal state with a short delay in breathing, which is necessary so that the so–called “iso-line” does not “float”, because even normal, not too deep breathing already strongly affects the blood supply to the brain, changing it and thereby causing a shift up and down the original recording line.
The recording in the middle is the state of blood filling of the cerebral vessels during the respiratory “Valsalva Test” – straining. Breath delay!
The bottom entry is the “Mueller Test”, the reverse of the “Valsalva Test” – the subject makes a maximum exhalation, followed by a strong maximum “inhale” movement, but NOT ALLOWING air to enter the lungs, and so holds the chest in this position for several tens of seconds.
Even a person who has never been involved in the diagnosis and analytical interpretation of curves is struck by the difference between these three records! The shape of the curves and their amplitude are clearly dissimilar!
Let’s do a light analysis of these records.
The leading edge of the wave of blood filling of cerebral (cranial) vessels is called anacrotum.
Posterior, descending – dicrotum. According to the amplitude of anacrotum, it is possible to judge how much the blood supply of blood vessels has changed under the influence of a wave of increased pressure (Systole) coming from the heart. That is, the clear space of the vessel, the degree of stretching of its flexible wall. Of course, the degree of wall stretching depends on its elasticity and on the pressure of the incoming systolic wave. If the wall is elastic and the cardiac output is normal, then the wall expands rapidly. If she has developed sclerotic changes that have reduced its flexibility-elasticity, then the anacrotume curve “creeps up” more slowly. A similar phenomenon can be caused by muscle spasm of the vascular walls. In the so-called “differential” diagnosis, which is designed to separate certain morphological changes in the wall from increased muscle tonus, a so-called nitroglycerin test is used. A very small dose of nitroglycerin is placed under the tongue of the subject. Nitroglycerin has the property that turns off the activity of smooth muscles in the walls of blood vessels, and thereby “cancels” its effect on the degree of pulsation of blood vessels. If the curve greatly changes its appearance, that is, it becomes sharp with pronounced elements of anacrotum and dicrotum, than the original shape of the REG, before the test, was caused by some kind of nervous increased vascular tonus.
If the shape practically does NOT change, it means that certain pathological processes (aging, for example) have developed in the walls of blood vessels, which have reduced its elasticity.
So, let’s start analyzing REG.
It is immediately obvious that the young subject is a typical neurotic, with a clearly overestimated tonus of the walls of the cranial vessels (vascular dystonia). Although his anacrotum is fast, but then the top of the curve is not sharp, but topped with some teeth. The last (far right) protrusion-tooth is called a dicrotumic tooth and it is generated by the end of systole, ventricular contraction, and the slamming of the aortic semilunar valves. The depression in the descending curve in front of it is called an incision, this is precisely the result of relaxation of the ventricular walls, a sharp drop in pressure in them and the slamming of the aortic valves.
In neurotics, a characteristic feature is a certain tooth at the top of the curve, called a PREINCISIONAL. With a nitroglycerin test, it disappears completely in young neurotics! It is caused by excessive and “inadequate” sensitivity of the vascular wall baroreceptors. They are triggered PREMATURELY by the build-up of a pressure wave in the blood vessels and, as a nervous reaction, contract before the pressure wave reaches its peak. On the upper “normal” REG, this is clearly manifested in the form of a “Three–pronged” vertex, where the last tooth is also a nervously “creeping higher” dicrotumic one, generated by a pressure wave in the stretched aorta after the valves are slammed shut.
This “preincisional prong” also appears in non-neurotics if, for some reason, the situation causes them even the slightest stress!!! A certain, albeit weak, “tension”!
On the second, middle recording, Valsalva’s probe, a strong change in the REG shape is visible. First, its amplitude has decreased by two times compared to normal. Why?
Because when straining, the intrathoracic pressure increases greatly and this reduces the venous blood flow to the heart. And according to Starling’s “Law of the Heart”, cardiac output directly depends on the degree of stretching of the wall of the relaxed ventricle. The more the walls are stretched, that is, the more blood has flowed from the atria, the stronger the subsequent contraction of the muscles of the ventricular walls. If there is little blood, then the discharge is less. What we see on the middle record.
But something else is also interesting here: The top of the curve is SHARP! Why? Precisely because the pressure wave is weak, it weakly stretched the “nerve wall” of the vessels and it DID NOT REACT to such a weak stretching by premature inadequate contraction! And the dicrotumic tooth became more pronounced and slid lower. Where he belongs!
The third, lower curve.
The most wonderful! With the Mueller probe, the reverse of the previous sample occurs. The intrathoracic pressure is low, the “discharge” in it is caused by the fact that the chest is raised by the muscles to the maximum, the diaphragm may also have descended lower and this created a kind of “vacuum” in the volume of the chest. As a result, the venous blood flow to the heart has greatly increased, all the vessels in the chest cavity have expanded due to the reduced pressure in it (the CORONARY ARTERIES HAVE ALSO GREATLY INCREASED THEIR DIAMETER!) and an increased amount of blood entered the ventricles, stretching their walls to the maximum. Therefore, the subsequent contraction of the myocardium was powerful and cardiac output increased several times! The wave of increased pressure reached the cranial vessels in a fraction of a second and caused their severe stretching. The REG amplitude has grown two to two and a half times!
BUT, the top has rounded suspiciously again! Not because of sclerosis, but because of the aforementioned excessive “nervousness” of the walls of the cerebral vessels! With some pressure, which has not yet reached its maximum, the smooth muscles of the vascular wall UNNECESSARILY worked, contracting, and thereby SLOWED DOWN the acute vertex stretching!
And the preincision prong appeared again and became more noticeable!
What to do if the subject, although young and healthy, is clearly neurotic, even at the level of the vegetative vascular reaction!
Faciant meliora potentes.
If I’m wrong, let my seniors correct me.
3 I 2026
